The document below presents an ideal UX approach, where extensive research, user interviews, the creation of detailed user stories, wireframes, and prototypes, as well as thorough user testing, would be essential. This approach allows for a deep understanding of the users and their problems, leading to a highly informed design.
However, this level of effort may not always be feasible in the real world due to time and resource constraints. Therefore, while this document outlines a comprehensive process ideal for any UX project, a more practical recommendation would be to implement the necessary components selectively, applying them as needed to address the most critical user needs at each stage of the project.
Table of Contents
- What’s the problem?
- What’s the business?
- Personas, Problem Scenarios, and Propositions
- Customer Interview Guide
- What problem are we solving? For who?
- Value Hypotheses & Testing
- Experiment Design (Customer Motivation & Engagement)
- User Stories & Prototypes
- Business Model Design (how do we test our user interface)
- Appendix A: Customer Discovery Notes
- Appendix B: Usability Testing
- Appendix C: Chain of Relevance Check-In
What’s the problem?
It is estimated that eight million Americans have an eating disorder; seven million women, and one million men. Eating disorders have the highest mortality rate of any mental illness. The National Association of Anorexia Nervosa and Associated Disorders reports that 5-10% of anorexics will die within 10 years of contracting the disease; 18-20% will be dead after 20 years, and only 30-40% fully recover. The mortality rate for anorexia in women is 12 times higher than the death rate for ALL causes of death for females 15-24 years old. After suicide, the primary causes of death for women with eating disorders is related to cardiac involvement.1
Around 80% of women who have accessed care for their eating disorders are discharged weeks before the recommended stay. The cost of outpatient treatment, including therapy and medical monitoring, can extend to $100,000 or more. Only one in 10 people with eating disorders receive treatment. The average cost for a month of inpatient treatment is $30,000. It is estimated that individuals with eating disorders need anywhere from 3-6 months of inpatient care. Rates of minorities with eating disorders are similar to those of white women.1
Hospital costs have reached over $41.3 billion for patients readmitted within 30 days of discharge. For Medicaid patients, the three conditions with the largest number of 30-day all-cause readmissions were mood disorders, schizophrenia, and diabetes.
For privately insured, the three conditions with the largest number of 30-day all-cause readmissions were maintenance chemotherapy, mood disorders, and complications of surgical or medical care. Readmission rates are 17.2% for 65+, 14.6% for 18-64 on Medicaid, 8.7% for 18-64 Privately Insured, and 10.6% for uninsured. For mood disorders, specifically for Medicaid, the readmission rate is 19.8%, 10.4% for Privately Insured, and 12.7% for uninsured.2
What’s the Business?
For [mental health professionals] who [provide counseling services for eating disorders], the [Hospital Readmission Reduction Application] is a [software application] that [reminds these professionals about follow-ups and provides guided paths to effectively follow up, including outpatient resources]. Unlike [current market products], our product [also monitors for readmissions to immediately put that client on the healthcare professional’s radar to help minimize their subsequent stays and medical costs].
Personas, Problem Scenarios, and Propositions
Note that there would normally be several Personas created for this type of application. This example will focus on two Personas.
Charlene the Therapist
Screening Question: Do you regularly provide mental health services that either require hospital admission or as a follow-up to hospital admission for eating disorder-related mood disorders? Save
 Charlene has been working as a therapist for over 20 years in the St. Louis, MO area, she focuses on BDD and eating disorders. She grew up with a mother who was very concerned with her daughters being thin, which caused her sisters to develop an eating disorder. Charlene watched as her older sister grew up with this disease, and she saw the negative impact it had on her family. As a result, Charlene does everything she can to stay healthy, she works out 3-5x a week at her building’s gym, she goes on morning runs around her suburban neighborhood. While she has no children of her own, she keeps up on child psychology issues as she’s learned that they tend to bleed into teenage and early 20s years and have a great deal of impact on eating disorders in adults. Charlene treats over 20 regular patients and provides in-patient services on-call for the hospital. She likes to avoid hospitalization for her clients as much as possible, but when it is necessary she has found that it is difficult to keep up with follow-up; and she is often dismayed to find out that a client has been admitted to the hospital without any notification by the hospital or client.
Charlene has been working as a therapist for over 20 years in the St. Louis, MO area, she focuses on BDD and eating disorders. She grew up with a mother who was very concerned with her daughters being thin, which caused her sisters to develop an eating disorder. Charlene watched as her older sister grew up with this disease, and she saw the negative impact it had on her family. As a result, Charlene does everything she can to stay healthy, she works out 3-5x a week at her building’s gym, she goes on morning runs around her suburban neighborhood. While she has no children of her own, she keeps up on child psychology issues as she’s learned that they tend to bleed into teenage and early 20s years and have a great deal of impact on eating disorders in adults. Charlene treats over 20 regular patients and provides in-patient services on-call for the hospital. She likes to avoid hospitalization for her clients as much as possible, but when it is necessary she has found that it is difficult to keep up with follow-up; and she is often dismayed to find out that a client has been admitted to the hospital without any notification by the hospital or client.
Charlene is technologically savvy but has found that performing administrative work takes up a considerable amount of time. For every hour she spends with a client she spends around an hour filling out notes and paperwork. This means that she works a lot of unintentional overtime as she really wants to provide her clients with the time they need, even if that means she stays late. She has a receptionist, but her receptionist is specifically for administrative work and not for any clinical work.
| Thinks | Charlene thinks that there should be some way to be notified when a client is admitted to the hospital immediately. Charlene thinks that there should be a way for her to provide better follow up services to her clients so she can watch for potential triggers that could result in a readmission. Charlene thinks that clients would do more to help themselves if it was more convenient than going to the office to see her. |
|---|---|
| Sees | Charlene sees that her clients have poorer outcomes the more they are admitted, that while they comply with hospital requirements while admitted, they revert further back upon discharge almost in defiance of what was done at the hospital. Charlene sees a higher suicide rate among clients who have had multiple readmissions. Charlene also sees how these eating disorders affect the friends and family members of her clients. |
| Feels | Charlene feels that the medical system caters to reaction vs prevention and she feels that her clients would benefit more from preventative care instead of reactive care. Charlene feels like she has failed her clients when they are readmitted. Charlene feels that the hospital doesn’t provide the right kind of follow up for the clients, so the clients feel abandoned upon release, are released too soon, and the families are left ill equipped to help their loved one. |
| Does | Charlene treats 21 clients on a regular basis at her practice, dedicating an 1-2 hours a week to each for personal counseling. Charlene spends approximately 10 hours a week at the hospital. She works an average of 10-15 hours of overtime each week. She would prefer not to work weekends, but she has worked every weekend for the past year. Charlene also makes additional time for the family and friends of her clients, which means that her schedule often runs late. Charlene takes messages and phone calls after hours as she wants to do whatever she can to prevent her clients from being readmitted. |
| Problem Scenarios | Current Alternatives | Your Value Proposition |
|---|---|---|
| Charlene has no way to provide the client with access to the notes she provides other than to give them a paper copy, so if the client loses the references she’s provided or the information she provides, they have no way to get it back without visiting her again. | CCharlene keeps notes of what she gave to the client but cannot take the time to make a copy, so if she needs to know what she gave them she has to search her notes. This means that she may give conflicting information or duplicative information. | Provide an application that allows the client to log in to see session notes, suggestions, and follow up resources. This application should make the notes searchable both for the provider and the client with separate areas for the provider only and for provider and client. |
| Charlene needs to be reminded at regular intervals to follow up with each client based on the client’s needs. | Charlene adds reminders in her Google calendar using codenames for each patient. She can’t use her practice’s calendar as it isn’t available on her phone. | Provide a HIPAA-compliant calendar within the app that, based on checkboxes on session notes and the client’s history, and of course, the therapist’s recommendations, will set up an automatic reminder schedule for follow-up. |
| Charlene doesn’t know all the resources available for her clients, or the best resources based on the client’s location and transportation abilities. | Charlene keeps a list of services she has experience with that she prints out and has available in her lobby and in folders in her office to retrieve for her clients as necessary. | Provide a customized list of resources based on a certain distance from the client’s preferred address. |
| Charlene cannot easily communicate with her clients to touch base with them between appointments, both due to time constraints and communication constraints. | Charlene asks her receptionist to call her clients to connect her between appointments, but she is only able to connect with clients less than 5% of the time. | Provide a forum type environment (think Slack), where the client can ask questions and get answers in a timelier manner than waiting for an in-person meeting. Embed video call capability. |
| Charlene doesn’t receive notification that a client has been readmitted until many hours, sometimes a day, after the readmission. | Charlene has no alternatives to this other than to wait for her clients to show for their appointments or receive notification from the hospital of an admission. | Enable the hospitals to share admission information immediately with the therapist via the app, that can automatically notify the therapist on their mobile device. |
Due to this being a sample, the above is a selection of several problem scenarios, many more would be drafted for this application.
Amy the Client
Screening Question: Do you currently receive therapy for an eating disorder?
 Amy is 17 years old and was diagnosed with an eating disorder when she was 11 years old. She is the middle child with an older sister and younger brother. She attends high school and was held back a grade due to low performance in grade 10. Her mother suffered from an undiagnosed eating disorder and through counseling she and Amy realized that she was putting her own insecurities onto Amy. Amy has been in counseling with Charlene for six years since her first hospitalization. She felt she was released too early and was quickly readmitted after relapsing.
Amy is 17 years old and was diagnosed with an eating disorder when she was 11 years old. She is the middle child with an older sister and younger brother. She attends high school and was held back a grade due to low performance in grade 10. Her mother suffered from an undiagnosed eating disorder and through counseling she and Amy realized that she was putting her own insecurities onto Amy. Amy has been in counseling with Charlene for six years since her first hospitalization. She felt she was released too early and was quickly readmitted after relapsing.
Amy enjoys playing soccer and going out with her friends. She likes comedies and thriller movies. She likes to read books about vampires and magic. She has dreams of becoming a doctor when she grows up. Amy works hard to stay on track and follow the plan Charlene has outlined for her but she feels like she’s just one of many in Charlene’s client list and feels ignored when she can’t get an answer until her next session. She feels like she can’t talk to her mom because her mom is part of the problem.
Amy is very technologically savvy and likes to use SnapChat, Instagram, Facebook, WhatsApp, and because she likes to make jewelry she likes to see what other people have done on Pinterest.
| Thinks | Amy thinks that the hospital doesn’t really understand what she needs. Amy thinks that Charlene doesn’t have enough time for her. Amy thinks that her mom is a big part of her problem. Amy thinks that she doesn’t matter much to anyone. |
|---|---|
| Sees | Amy sees that her mother needs her own counselor because she still has issues at home. Amy sees that the hospital cares about money more than her therapy. Amy sees how much it stresses out her mother that she’s still in therapy. Amy sees how her eating disorder is affecting her life when she has to cancel activities. |
| Feels | Amy feels neglected and abandoned. Amy feels like she is getting generic answers and care from Charlene. Amy feels like she has no control over her therapy or resources because she doesn’t have a car so she has to rely on her mom. Amy feels lonely and ignored when she has no one to talk with. Amy feels like she needs more than one session a week. |
| Does | Amy has therapy sessions weekly with Charlene. Amy tries to look into the resources given to her but is limited by her mobility. Amy looks up nutritional information online because she doesn’t have access to a nutritionist. |
| Problem Scenarios | Current Alternatives | Your Value Proposition |
|---|---|---|
| Amy has no way to communicate with Charlene outside of their scheduled sessions. | Amy can ask for more appointments. | Provide an application that allows the client to log in to see session notes, suggestions, and follow up resources. This application should make the notes searchable both for the provider and the client with separate areas for the provider only and for provider and client. |
| Amy doesn’t hear from Charlene between sessions for follow-up to see how she is doing or if she needs anything additional. | Amy goes online and looks up help boards and forums, which can provide incorrect information. | Application allows Amy to request chat response or follow-up by a variety of means including virtual sessions if she is unable to get to the office.. |
| Amy isn’t able to keep track of all of the resources provided by Charlene or get to them because some of them are too far away. | Amy has a folder to put the resources in but she can’t easily find what she needs. | Provide a customized list of resources within walking / biking distance and within driving distance for Amy within the app and make the resources searchable and sortable. |
| Amy feels alone when she is readmitted to the hospital as it tends to happen on the weekend or on a holiday and between sessions and Charlene doesn’t find out until many days later. | There are no current alternatives for this situation, Amy has to wait until the hospital notifies Charlene. | Enable Amy to notify Charlene immediately that she is going to be admitted so Charlene can act immediately. Provide notification to Amy that Charlene has been notified of her intake. |
Due to this being a sample, the above is a selection of several problem scenarios, many more would be drafted for this application.
Customer Interview Guide
Screener
Do you regularly provide mental health services that either require hospital admission or as a follow-up to hospital admission for an eating disorder
related mood disorders?
Persona Hypothesis
- Tell me about [yourself in the role of the persona]?
Tell me about being a therapist? Why did you choose to become a therapist? What do you like most about the job? What do you like least? What are the hardest parts of your job? What are the easiest? - Tell me about [your area of interest]?
Tell me about your current process when you get a new client. Tell me about the process you follow when called to the hospital to see a new client. Who all is involved in the intake of one of your clients? How do they communicate with you? How do you communicate with your clients? - Tell me your thoughts about [area]?
How are things done now vs. how would they work in a perfect world? What have you seen work well vs not well for following up with clients after hospital admission? What contributed to the best outcome you’ve experienced? What contributed to the worst outcome you’ve experienced? - What do you see in [area]?
Where do you learn what’s new in mood disorders and treatment? What do others do? Who do you think is treating mood disorders most effectively? What programs do you know of that are doing the best job with mood disorders? - How do you feel about [area]?
What do you feel about hospital practices regarding eating disorder discharge policies? What motivates you? What parts of providing therapy are most rewarding? Why? How do you feel you can do better for your clients? - What do you do in [area]?
What do you do in your practice to help prevent hospital readmittance? What do you do to keep in contact with your clients? How many hours did you work last week? Is that typical? What are your favorite online tools to use? What are your favorite resources to give to your clients?
Problem Hypothesis
- What are the top [5] hardest things about [area of interest]?
What are the top 5 hardest things about providing therapy? Why? What are the top 5 hardest things about providing care at the hospital? Why? - What’s [difficult, annoying] about [area of interest]?
What’s difficult about providing therapy? What’s difficult about following up with your clients? What makes it difficult to communicate with your clients after therapy? What annoys you about the current process at the hospital for intake and discharge? - How do you currently [operate in area of interest]?
How do you currently communicate with your clients between sessions? How do you currently share information with the friends and family for how they can support their loved one? How do you communicate with the hospital about your clients and how do they communicate with you? Who communicates with you? - What are the top 5 things you want to do better this year in [general area of interest]?
What are the top 5 things you want to do better this year for your clients in your practice? What are the top 5 things you want to do better this year for your practice at the hospital? - Why is/isn’t [your specific area of interest on that list]?
Why isn’t [X] on that list?
Closing and Miscellaneous
- Casting a Line (“Anything else?”)
- Housekeeping and Follow-up
What problem are we solving? For who?
What job are we doing for who? How do we know if it’s working?
‘A certain therapist exists, and she needs to lower her clients’ hospital readmission rate. Currently, she tries to keep up with her clients during her off hours, but if we offer her a program that will utilize the information from her sessions to recommend a follow-up schedule and resources, and that will enable her to keep an open line of communication with her clients, then we’ll observe a lower hospital readmission rate for her clients, and fewer fines for the hospital on readmissions for their clients.
Value Hypotheses and Testing
What is the core value hypothesis?
If we provide therapists with a tool for communication with the hospitals and their clients, then they will try it, buy it, standardize on it, and it will improve hospital readmission rates and client outcomes with therapy.
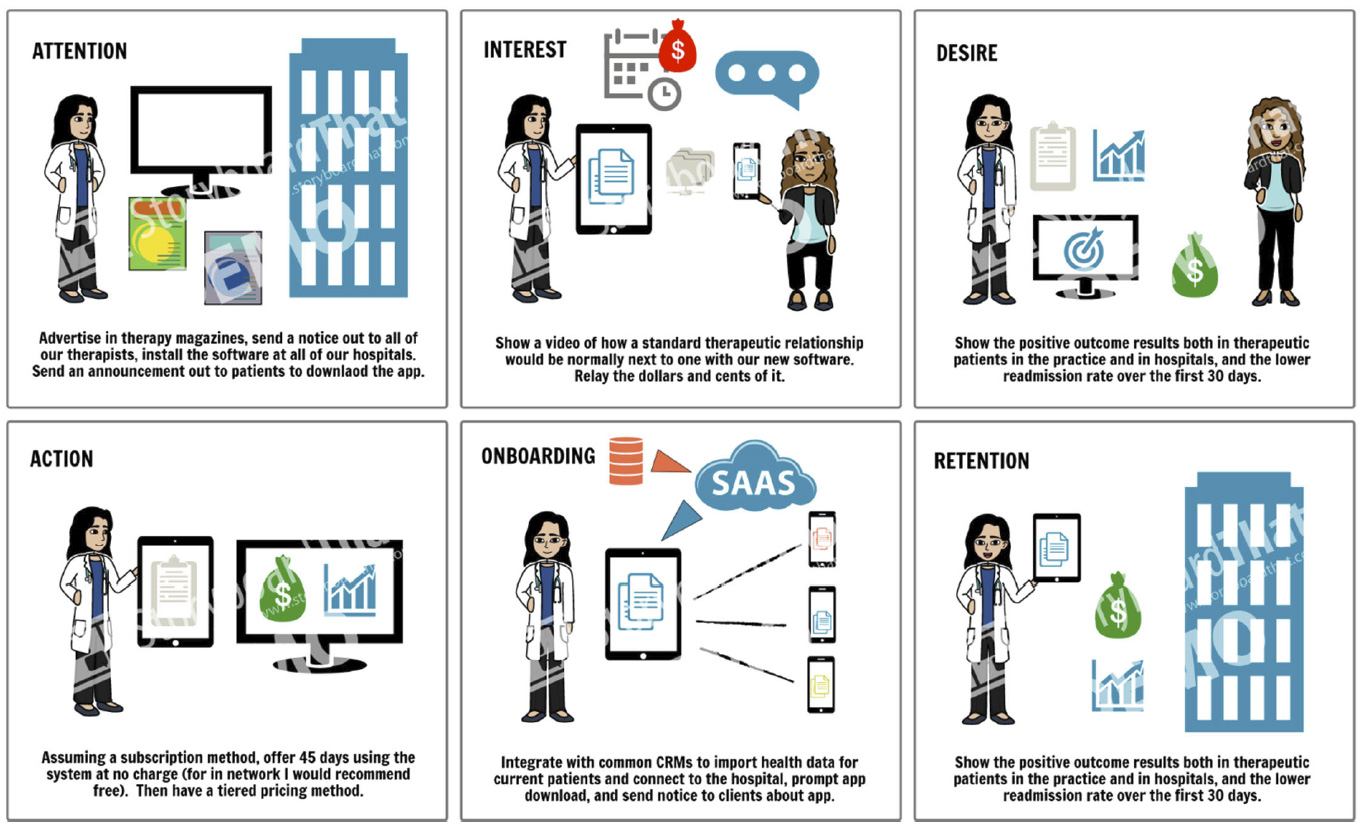
What is the customer journey?
Testing
| Item | Acquisition | Onboarding | Engagement | Outcome |
|---|---|---|---|---|
| What does this mean? | How do we get therapists and hospitals to start using our new software application? How do we get clients to start using it and trust that their data is safe? | How do we make the transfer of client information as painless as possible? How do we notify clients to download the app or access the website? | How do we keep the therapists and hospitals engaged in using the software? How do we keep clients engaged with using the software to interact with their therapist? | Ideally every therapist and hospital in our network would be using the software by default to minimize the acquisition factor from “should I” to “I wish this was around sooner.” |
| What is the interval for an observation? | 45 days is sufficient time for all of the users to quantify a measurable positive gain. | 1 day for therapists and 1 day per department for hospitals. That is a reasonable amount of time for data conversion (not including time to create the conversion protocol). | Make it effortless to keep the users excited about participating and using the software. | No effort required for the therapists or hospitals to load patient data, seamless integration to instantly begin notifying therapists and sharing data with their clients. |
| How might we test this? | Calculate how many therapists and hospitals signed on for the software trial and verify app installs. | Calculate how many therapists and hospitals requested data conversion. | View statistics on usage by day and hour and duration of use by each type of user. | Measure hospital readmissions over a similar period with similar patients. Survey clients for their satisfaction. |
| What are the metrics? | Number of Therapists Number of Hospitals Number of Clients |
Number of Users who request data conversion. | Number of users still interacting on a daily basis at 15 days, 30 days, and 45 days. | Number and cost of readmissions over the 45 day period AND the 45 days after that period. |
| What’s tricky? What do we need to watch out for? | Reluctance to try something new. Fear about data security. Reticence about time required to learn this new technology. | Fears about time for data conversion. Data conversion with a system we aren’t familiar with. Clients without electronic devices capable of viewing and using the app on a computer or mobile device. | Engagement slipping without constant reinforcement of usage. | Cessation of use after 45 days. Higher readmissions during this time period. Outside influence that could cause higher readmissions unrelated to the use of the software. |
| How can we combat or prevent the potential issues? | Offer a variety of training options (manuals, online, webinar, in person) and have the software extraordinarily intuitive. | Be ready with conversion scripts for the most popular CRMs and EMR systems. | Provide constant feedback about interactions, client usage of the application to the therapist AND therapist interaction with the application for the client so they can see that the therapist is using it and that it is not an afterthought. Provide valuable and actionable information immediately to all parties. | Check in with users every 5 days to see what could be done better and release those upgrades within a week whenever possible. Monitor outside influences that could negative affect readmissions and warn therapists and hospitals about them and their risk factors to help them to take preventative action vs reactive. |
What are the key assumptions/hypotheses?
This is an ‘unpacking’ of the core hypothesis above. How did our customer get to the happy place where they’re a regular user of our product? How did they find out about it? How did they buy it? When/why do they use it? How often do they use it?
| # | Priority * | Assumption / Hypothesis | Needs Proving? | Experiment (MVP) Vehicles, Metrics, and Notes |
|---|---|---|---|---|
| 1 | 0 | If we provide software that allows a therapist to be notified when a client is admitted to a hospital within 30 days of their previous admission, then they will be able to react faster and reduce that client’s stay and thus their cost. | Yes | Track number of readmissions within the 90 day time period of the start of use of the application and the cost of those readmissions compared to previous readmissions of the same and similar patients. |
| 2 | 1 | If we provide the ability for therapists to communicate with their clients electronically, then they will be able to quickly react to client communication without waiting for an appointment and will be able to provide better follow-up. | Yes | Provide a questionnaire to the therapists and the clients regarding communication and their opinions on the time spent on it and whether or not it is valuable and if they wish they had more communication and what means that communication should employ. |
| 3 | 2 | If we provide a program that can target resources based off checkboxes and selections by the therapist for a client, that are based on their geographical location and transportation means, then the client will have better resources to utilize. | Yes | Request the resources that therapists have provided to their clients and pool them from a variety of therapists and share that information between them to see if it is valuable to see what the value would be of a shared resource component of the software. |
| 4 | 2 | If we provide clients with a web app and native app that they can use to pose questions to their therapists 24/7 and access notes and resources from their therapists at any time, then clients will no longer feel abandoned and will have a longer time between hospital readmissions as they will be able to utilize the resources more effectively. | Yes | Question the clients about their interactions and ask what types of interaction they would prefer, what timeline, what they feel is missing from their therapist relationship. Question the clients about the resources they use that the therapist has provided to them. Question the clients about the accessibility and usefulness of the resources provided and if they have found any of them to be more or less effective. Provide a rating system for resources. |
Rating Scale
0: This is our core/summary value hypothesis.
1: Pivotal hypothesis. If this is disproven, the venture needs to be canned or go through a fundamental pivot.
2: Child detail of a pivotal hypothesis.
3: Child of above.
4: Extremely important hypothesis. This hypothesis substantially affects key profit drivers.
5: Important hypothesis. This hypothesis affects key profit drivers.
6-10: Tactical hypothesis for incremental improvements in various areas.
X: Not sure of the priority of this hypothesis.
Experiment Design (Customer Motivation and Engagement)
Client Communication and Access to Data
| What hypothesis will this test? | If we provide clients with a web app and native app that they can use to pose questions to their therapists 24/7 and access notes and resources from their therapists at any time, then clients will no longer feel abandoned and will have a longer time between hospital readmissions as they will be able to utilize the resources more effectively. |
|---|---|
| How will we test it? | The experiment will include a beta set of users from a select group of therapists over a 14-day time period. We will preload the app with those clients’ data and have the therapist set aside 30 minutes each day to interact with the clients via the app in two 15 minute or three 10-minute increments to allow for multiple touch points. We will acquire subjects by having the therapist identify individuals in their practice that would be willing, we would provide a brochure that they can give to clients and the ability for them to give access to the app immediately (research has shown that if someone downloads a app immediately and starts to use it within the first hour that they will have a greater chance of continuing usage). We will design the full communication experience to send questions, receive answers, view previous notes and resources, and look up other recommended resources by other clients and therapists. |
| What is/are the pivotal metric(s)? What is the threshold for true (validated) vs. false (invalidated)? | The pivotal metric will be the level of usage as the days go on and the response time for the therapist to respond to the client and their response time in reaction to the therapist’s communique.
Validated threshold would be at least one usage every three days during the 15-day time period. Even if it is just a touch point from the therapist to the client providing encouragement. We should be able to monitor if the client views the information from the therapist. Even if they don’t respond. Note that all actual information will be confidential, we will only see if something was sent and the therapist can categorize it as a conversation, response, resource, or encouragement, and if the client reacted to it. |
| What will you do next if the result is true? False? | If validated, then we will move onto asking for feedback to make the application better for both parties and release it to a greater audience.
If invalidated, then we will ask the therapist and clients what didn’t work and how we can make it more useful and effective. |
| How much time, money will it take to set up? | To set up the experiment it will take: – [$] and [y] hours of writer time. – [$] and [y] hours of design time. – [$] and [y] hours of development time. – [$] and [y] hours of architect time. – [$] and [y] hours of marketing time. – [$] and [y] hours of training time. |
| Roughly, what will it take for each individual test? | For each test it will take [$] and [y] hours for team interpretation. |
| Roughly, how long will it take for each test to run and produce definitive, actionable results? | Each test will take 15 days to produce results. We can extend this to 30 days if we find that is necessary. |
Experiment Results
| Did the experiment work? | |
|---|---|
| What was the sample size and the results? | |
| Conclusions? |
User Stories and Prototypes
User Stories
If we provide a program that can target resources based off note contents, checkboxes, and selections by the therapist for a client, that are based on their geographical location and transportation means, then the client will have better resources to utilize.
| Story | Notes |
|---|---|
| As a therapist I want to be able to enter my notes for each client quickly without having to go to the client’s profile, so that I do not have to click more than a few times to get to this feature so I do not lose my train of thought. | Combo box type ahead drop down by user short-name, nickname, full name, medical ID, or other identifier as identified by the therapist as useful (including smart suggestions by appointments that day if around a specific time). |
| As a therapist I want to be able to write specific phrases using hot keys, so that I can save time writing repetitive phrases. | Have a hotkey creation screen where the therapist can enter the phrase and the hotkey that would be pressed to trigger it or the words (think iPhone short phrases). |
| As a therapist I want to be able to have a common selection of checkboxes for follow-up protocol based on diagnosis, so that I can automatically set up follow-up triggers with clients to provide better engagement and support. | Work with the therapist to discover what follow-ups are common for situations and allow them to create these combinations by setting up the notifications they and/or the client will receive when each of these is checked. |
| As a therapist I want to be able to view a resources screen based on my client’s preferred geographical location, so that I can refer them to resources that are accessible for them. | Integrate Google mapping to allow for map-based resources added by the therapist and recommendations from other therapists. Allow the therapist to easily select those resources and forward them to the client’s portal with a note. |
| As a therapist I want to be able to see my client’s opinions of the resources that I provide to them, so that I can better recommend resources in the future. | Allow clients to rate and provide comments on the resources to make them better for all clients. |
| As a therapist I want to be able to provide take-away resources with a click, so that my clients can have 24/7 access to any printable resources I have provided. | Allow therapist to add worksheets and documents via upload to a private portal, links to documents within the portal, and links to documents and apps outside the portal. |
| As a therapist I want to be able to identify if I’ve provided a resource previously to a client, so that I don’t send it again. | Indicate by a symbol if the resource has already been sent to that particular client. Allow the therapist to prompt the client with the information again in a single click. |
| As a therapist I want to be able to search all of the resources by keywords, address, specialty, so that I can easily find resources that are not in the short list. | Provide a google like search through the resources area of the application. |
| As a client I want to be able to see all of the resources the therapist has provided me grouped by various factors, so that I can easily find the resources I need when I need them. | Provide a car like search with filtering and ordering using something like datatables to allow the clients to easily filter the list of resources provided, also indicating if they’ve accessed the resource previously. |
| As a client I want to be able to fill out resources inside the application, so that I don’t have to find somewhere to print it and so that my therapist has immediate access to my responses. | Make any forms or documents online forms that can be saved mid process, with automatic reminders to complete, and with the ability to include video files, photos, or other uploads as deemed necessary by the client and therapist. |
| As a client I want to be able to leave notes and a rating on resources that my therapist recommends, so that she understands what works well for me. | Provide a notes area and rating area for each resource so that the client can rate and remark on resources for better experiences. Allow the client to leave notes on every resource multiple times as they may use it multiple times so it may be effective one time but not another time. |
Due to time constraints, this is an example of some user stories that could be used to develop the software prototype for this aspect of the application.
Comparables
Note that this section is incomplete for this demo purpose but would be helpful for an actual product.
 TherapyNotes – Therapynotes.com
TherapyNotes – Therapynotes.com
- Schedule appointments within or allow clients to schedule appointments.
- Document session with easy to use templates and to do lists.
- Create bills and submit insurance claims.
 TheraNest – theranest.com
TheraNest – theranest.com
- Easily create notes, progress notes, initial assessments, treatment plans.
- Sign, approve, and co-sign notes.
- Integrated with common HER applications and planner applications.
- Automatic templates for notes.
 SimplePractice – simplepractice.com
SimplePractice – simplepractice.com
- Access to notes, scheduling, and billing in one application.
- Fully paperless client intake.
- Send secure, HIPAA-compliant messages to/from clients.
- Schedule appointments easily with online booking.
- Lets clients upload documents.
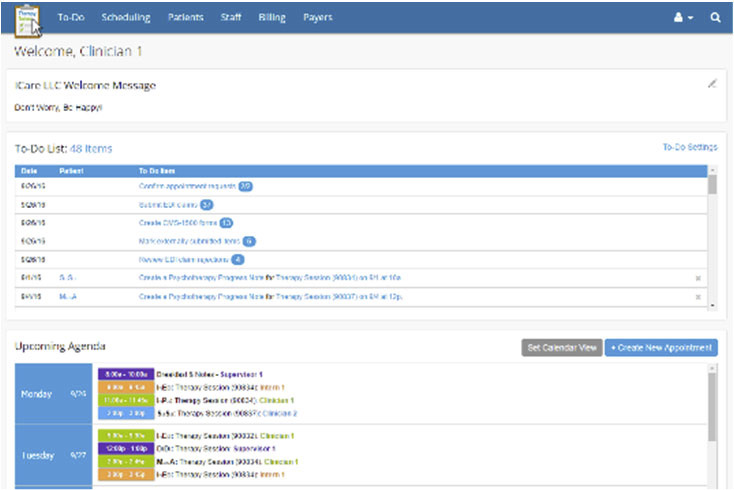
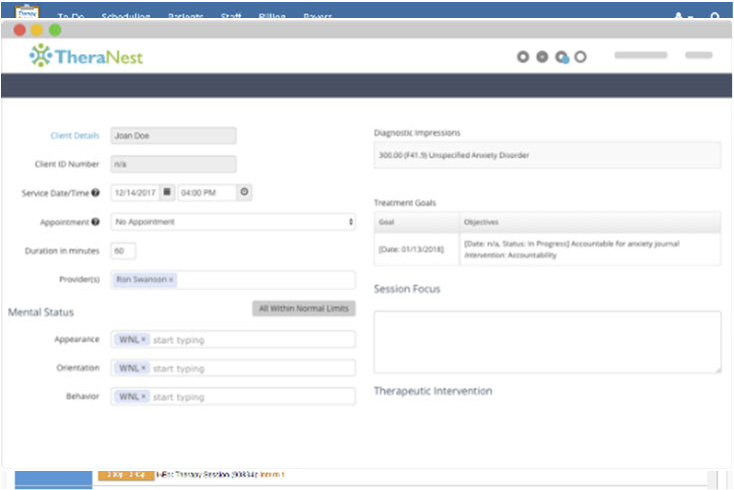
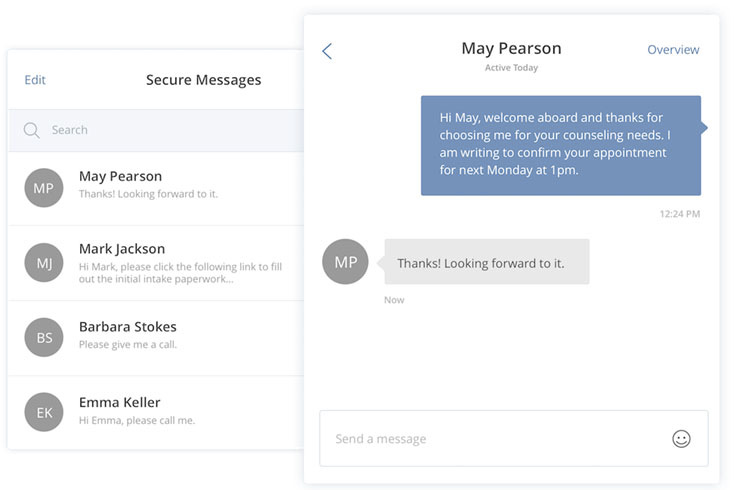
Prototypes
Concept 1 (therapist view on iPad, client view on iPhone)
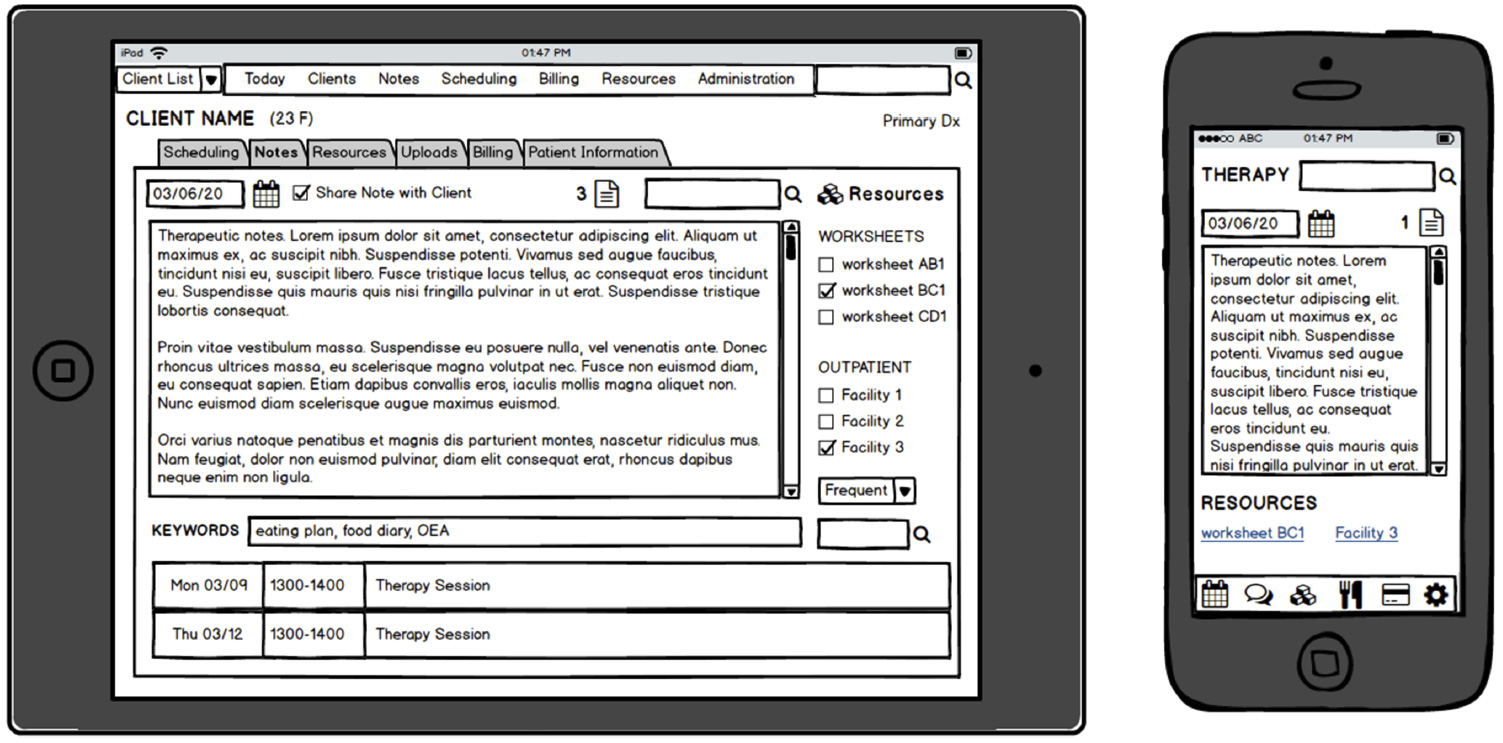
Note: this is a single quick mockup for this example, an actual project would contain several mockups and wireframes for all aspects. This is an idea of the type of wireframes that could be provided.
We could move to higher fidelity wireframes for a clickable prototype. (this is just an example of a health app, not necessarily this app)
Business Model Design (How do we test our UI?)
Key Partners
– Therapists
– Hospital IT
– Hospital Nurses
– Clients
– Input of client data.
– Sharing of client data between hospital and therapist.
– Sharing resources and data from therapist to client and vice versa.
– Client feedback to therapist.
Key Activities
– Searchable notes with keywords and associated resources.
– Resource feedback.
– Chat / forum capability for therapist and client.
Value Propositions
– Ability to be notified immediately of a hospital readmission.
– Ability to communicate quickly and effectively with clients in a means that works for them.
– Ability to share appropriate resources with clients. Ability to receive feedback on resources.
– Ability to search notes by both therapist and client.
Customer Relationships
– Therapist to Hospital
– Hospital to Therapist
– Therapist to Client
– Client to Therapist
Customer Segments
– Therapists
– Clients
– Hospitals
– Insurance Companies
Key Resources
– Client data from therapists
– Client data from hospitals
– Client input from client
– Resource data from therapists and clients
Channels
Digital applications available on computer and all forms of mobile device (indicates a web app approach).
Cost Structure
– Research, Design, and Development.
– Server, database, and hosting.
– Ongoing maintenance.
– Application integration with EHRs and CRMs.
Revenue Streams
– Lower hospital readmission rates = fewer fines for therapists and hospitals.
– Based on research therapists would be willing to pay up to $X per month per client.
Appendix A – Customer Discovery Notes
Visit Charlene’s Office on March 3, 2020
- Audience: Charlene T.
- Venue/Circumstance: 1234 Main Street, Suite 202, 63108
- Notes on the Persona: [What was on their A-list? What were they like? Think-See-Feel-Do?]
- Notes on Problem Scenarios: [Which ones did they have? What alternatives? What value propositions might resonate?]
- Insights on Personas and Problem Scenarios: [How did the interview prove or disprove key hypotheses on your personas and problem scenarios? How else did they change your point of view?]
- Other Insights: [add notes]
Note: This would be repeated for each custom discovery.
Appendix B – Usability Testing
Charlene Therapist – Exploratory Testing
Objectives and Methods: Therapist should be able to add a new patient (or import from EHR), schedule a recurring appointment with a specific number of recurrences, be able to add private and shared notes to a client’s record, select resources to share with the client, add a new resources, map resources to the client’s preferred address, view chat requests from the client, respond to chat requests, view ratings on resources by the client, perform admin capabilities (summarized for brevity).
Product Version: Version 001.01
Subjects: Charlene T. – Therapist – See Personas
Pre-Session Checklist
- Therapist account active: username and password sent to therapist.
- Therapist data imported: Confirm with therapist that data import was successful.
- Prototype able to achieve all activities above (these would normally be broken into individual test items): Confirm by walking through test plan.
Session Design
This is where a full explanation of the software would go with its benefits and an outline of the features it contains. This would include a walk through tutorial of how to use the software in the most basic terms (potentially have the client watch a video so the experience is consistent from therapist to therapist and client
to client).
Test Items
| # | Research Objective | Est v Actual (min) | Notes |
|---|---|---|---|
| 1 | Add a new client manually or by importing from EHR. | […] | Moderator Guide: … Output: …. |
| 2 | Schedule an appointment for the new client. | […] | Moderator Guide: … Output: …. |
| 3 | Add a private note for an existing client. | […] | Moderator Guide: … Output: …. |
| 4 | Add a shared note for an existing client related to a previous appointment. | […] | Moderator Guide: … Output: …. |
| 5 | Add a new resource and assign it to a diagnosis. | […] | Moderator Guide: … Output: …. |
| 6 | Select 1-3 resources for an existing client. | […] | Moderator Guide: … Output: …. |
This is a selection of tasks only.
Takeaways from Therapist – Charlene T. 03/02/20
Personas and Problem Scenarios
She spoke quite a bit about her frustrations with the current system and how she couldn’t just import them from the EHR that already contains all the information she needs. She shared stories about recent client readmissions and how difficult it was for her and her clients and how long it took the hospital to notify her and relay information to her client. This would continue with extensive notes from each person in attendance at the session as each person would have a different perspective and would notice different things during the meeting.
UI and User Stories
Charlene was able to enter a client within minutes by importing from her EHR. She wasn’t sure how to use the global notes search feature initially but once she tried it she found it much easier to find the information she was looking for. This would continue with notes about each user story and notable successes and failures.
Post-Test Debrief and (optionally) Footage
This is where a link to a screen recording would go.
Appendix C
Project Retroc/Check-In
This template is for a quick check-in as we’re focusing our work toward some future output, be it a product or promotional iteration.
| Item | Notes on Diagnosis |
|---|---|
| PERSONA CHECK Can we find 10 people that will love the product? Could they lead to 100 more? Then 1,000? Do we know how they relate to our area? |
Therapist and client pairs exist throughout our network. Hospitals that refer to our therapists also exist throughout our network. We would not be limited to our local area; this application could be nationwide and would also facilitate when clients move throughout the US. |
| PROBLEM CHECK Does our problem matter enough? Do we hear it as a response to open-ended questions? Do we understand the alternatives in detail? |
We do hear that fines and additional costs are a problem for hospitals and insurance companies. We do not hear about fines from therapists but rather we hear about lack of ability to mitigate and prevent readmission and the lack of communication from the hospitals upon their clients being readmission. We hear from clients that they are lacking communication between therapy sessions from their therapist and that some of the resources given to them are inaccessible. |
| VALUE HYPOTHESIS CHECK Do we have a tightly defined proposition? |
Our core value hypothesis is: If we offer therapists, hospitals, and therapy clients an application that allows them to communicate better and more often, hospital readmission rates will decrease for mood disorders.
We think this is the right scope and focus to deliver on the problem and loans itself to rapid, high-value testing. |
| VALUE DISCOVERY CHECK How can we test it in the next 48 hours? |
For a quick test, we think a concierge test with a variety of therapists will allow us to test the core value hypothesis and better understand the three primary personas that are expected to interact with they hypothetical product. |
| PRE-DEV CHECK Do we really need SW to move forward? Are we ready to narrate what the project needs? Test it often to avoid waste? |
If we offer therapists a program that will utilize the information from their sessions to recommend a follow-up schedule and resources, and that will enable them to keep an open line of communication with their clients, then we’ll observe a lower hospital readmission rate for their clients, and fewer fines for the hospital on readmissions for their clients We’ve defined the building blocks we need for this and looked at comparables and UI patterns. We need to describe the functional experience we want the user to have. |
Post-Mortem
- What was the execution and what constituted success/validation? What actually happened?
We’re building a new application for therapists and we hope to see 90% of the therapists add an item to an
existing client or add a new client within three days of signing up for the application.
Out of 24 signups, 92% added an item to an existing client’s record in the system and 10% added a new client
(note that all therapists had their data imported so it was not expected that many would add a new client),
and 20% of hospitals used the system to notify a therapist of a client’s readmission.
This validates our hypothesis. - Did our testing predict our outcomes?
- At a high level, I like to divide up testing into work that delivers on three main buckets-
- Persona & Problem Hypothesis: Discovery interviews & observation.
- Value Hypothesis: MVP & other product proxy testing.
- Usability Hypothesis: Product usability against specific (supplied) goals. Persona Hypothesis: after interviewing 24 therapists and four hospitals for the provider personas, we have a consistent set of perspectives and points of view. We believe that we have a solid foundation and validation of what is required in our software offering to help reduce hospital readmissions.
- Problem Hypothesis: we have consistently heard from Therapists that they have issues providing on-going communication with their clients between sessions and after release from an inpatient program. We have consistently heard from clients that they feel abandoned when their therapist isn’t notified for days of their admission. We have heard consistently from hospitals that readmissions are on the rise, especially due to social media bullying issues and media influences, and that they are willing to do what they can to help therapists provide better care.
- Value Hypothesis: We have performed two MVP vehicles to test our value hypothesis. The first was our concierge MVP where we worked with the therapist to provide immediate access to resources based on client location, adding notes for ease of use by clients and therapists, and searching of notes … this is where we would detail everything about our testing methods we used to validate our hypothesis to move forward.
- Usability Hypothesis: We moved from exploratory to assessment to validation testing with the V 001 interface. 100% of the subjects were able to add information within the first three minutes of using the application. Testing vs Actuals: We would want to summarize our testing vs actuals results here to see where we need to focus on refinement.
- What understanding we were implementing?
- The stories and wireframes outline on pages X and X outline the understanding that we are trying to test.
- What were the key propositions? Hypotheses?
- We would outline the key propositions and our hypotheses here.
- What problem were we solving? Was it important? Better than the alternatives?
- We would outline our problem scenarios and alternatives
- Who were we doing this for and do we know what makes them tick?
- We have two principal personas:
- Charlene the Therapist and Amy the Client.
- Charlene’s key motivation is to allow for better follow up and communication with Amy through an application that allows for text and visual communication outside of the therapy sessions. We believe that our product’s ability to allow that communication will be the pivotal reason for Charlene to use our software. Amy will see substantial benefits once the therapist starts to interact with the application, and she interacts in return. Amy will see mood and control increase based on the availability of information from Charlene outside of their scheduled appointments.
- We have two principal personas:
Footnotes
1. South Carolina Department of Mental Health. (n.d.) Retrieved from https://www.state.sc.us/dmh/anorexia/statistics.htm
2. Hines, A. L., Barrett, M., Jiang, H. J., Steiner, C.A. (2014, April). Statistical Brief #172. Retrieved from https://www.hcup-us.ahrq.gov/reports/statbriefs/sb172-Conditions-Readmissions-Payer.pdf
